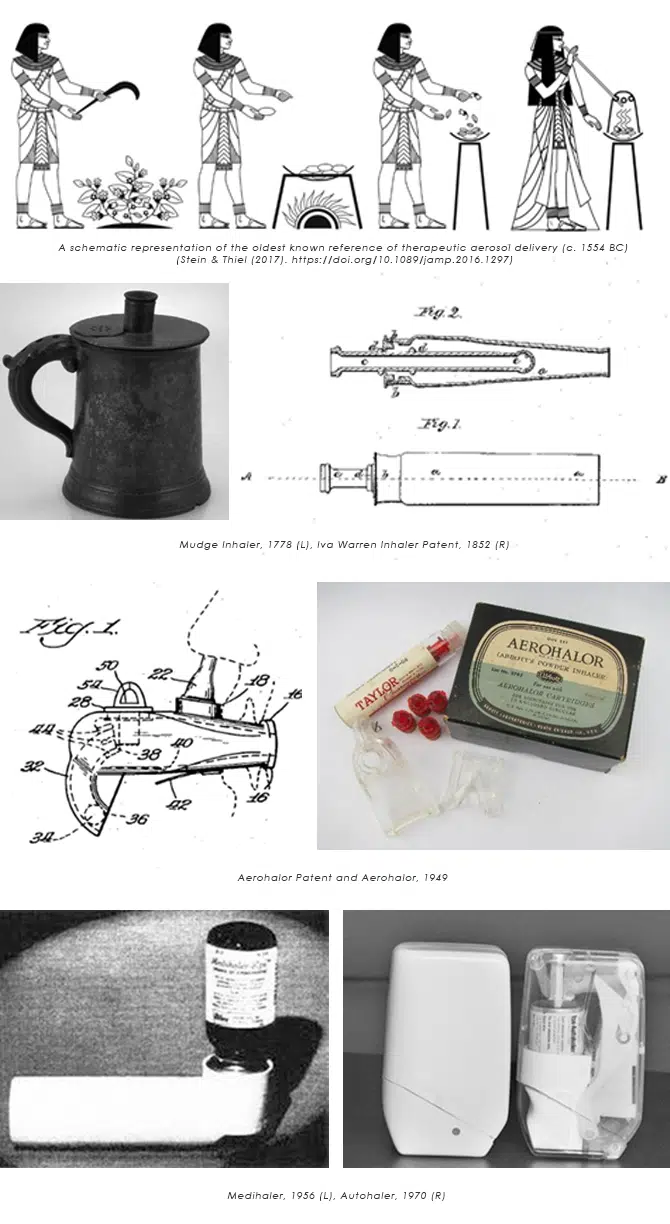
Inhaled medicine can trace its roots back throughout human civilization to the ancient Egyptians. On an ancient papyrus scroll, there is a depiction of people with breathing difficulties inhaling the vapor formed when black henbane plants were placed onto hot bricks. A jar with a hole was then placed over the herbs and the fumes inhaled through a stalk of reed that was placed into the hole.
Fast forward to the industrial revolution, dedicated inhalation devices started to appear thanks to advances in knowledge of respiratory illnesses as well as the production of medicines and devices.
Initially, ‘inhalers’ we more like modern-day nebulizers in that the user would inhale medicated vapours from aqueous solutions, often following a heating operation. The first known commercialisation of an inhaler was the Mudge inhaler. Released in 1778, it was a pewter tankard with a flexible mouthpiece and valve that allowed the user to breathe in and out without taking their lips off the mouthpiece.
Following this initial innovation, inhalers continued to develop throughout the 19th century. The first dry powder inhaler (DPI) was invented in 1852 by Ira Warren. It was a glass inhaler with an inner tube and small holes at the end that the medicine would be placed inside. The inner tube would be spun while the user breathed in through the mouthpiece. Atomisers and the first nebulizers we also developed during this time. As advancements in rubber manufacturing continued throughout the early 20th century, new types of atomizers using rubber bellows began to exist.
The first commercially successful DPI, the Aerohalor, was invented in 1949. It had a steel ball inside that moved when the user inhaled to disperse the powder and the patient could inhale through the nose or mouth. It was quite inefficient at dispersing the drug to an inhalable form.
The first metered dose inhaler (MDI) was created in 1956 by Riker now (3M Laboratories), it was a breakthrough in the treatment of Asthma and COPD. The Medihaler was initially released with two drug options (epinephrine and isoproterenol). The development of this MDI allowed for a wider variety of drugs to be tested and released with an inhaler.
Due to its success, the MDI is synonymous in minds in the UK as a ‘normal’ inhaler. Industrialisation continued to push devices forward and the industry scaled massively during this time as the cost of components and price to the user reduced, improving access.
One of the primary challenges of the MDIs at this time was that some patients have difficulty synchronizing releasing the dose and inhaling. This created a drive for breath-actuated inhalers. The Autohaler was the first breath-actuated MDI, commercialized in 1970 again by Riker to moderate commercial success.
An additional major development for MDI medication was Salbutamol (Ventolin) which was commercialised in an MDI in 1981, Ventolin can now be provided in both MDI (Evohaler) and DPI (Accuhaler) form.
Due to concerns about CFCs and the 1987 Montreal pact, the drive for the development of DPIs returned, and companies such as Glaxo-Wellcome (GSK) came up with new mass-produced DPIs which removed the propellent in favour of a powder inhaled from a sealed blister – unsealed by the device. The Diskus is the most commercially successful inhaler currently and returns several billion per year in revenue. The Diskus form was, and is, a huge success in this space due to it being breath actuated and offering dose control and counting. Due to its design, it has only been proven as a good platform for a handful of treatments.
The Montreal pact also pushed forward the shift from CFC to HFA propellants in MDIs, and more generally kicked off a wave of innovation in the space, with new patent families going through the roof.

Today the inhaler space is vast, providing relief for asthma, COPD and many other illnesses. There are countless mechanisms and designs due to the unique challenges that delivering different treatments bring.
MDIs are still extremely common and with the expiration of patents for some of the best treatments, universal platforms are slowly becoming more common. The regionality of regulations means that certain devices have become more popular in Europe as opposed to the US or East Asia.
But what does the future look like? Research shows that in the UK, around 12 million people are affected by lung disease and the number will grow as the population increases. The 2022 Asthma UK patient survey also revealed that 30% of users did not pass the technique test, suggesting inhalers are used not in an optimal way, leading to poor outcomes and avoidable deaths.
Connected inhaler add-on devices such as PropellerConnect from Propeller Health and FindAir have entered the market and smart inhalers will continue to do so. This allows for that dose tracking and the quality of the self-administering of each dose can be measured so that health professionals could offer alternative inhaler options to suit a customer or provide feedback on how to improve their inhalation method.
The reusability of inhalers is likely to be more and more focussed upon to take environmental issues, there will be a steady decline in MDIs to DPIs. We also expect to see continued variation in methods of inhalation as the device space is seeing continued rapid growth, and various drugs require various types of delivery platforms so reservoir, blister tape, or blister insert inhalers will continue to develop as different pharma companies try to find their niche and space in the market.
More than 85% of patients and carers support the use of more environmentally friendly inhalers according to a 2021 European respiratory journal survey. HD predicts to see an increase in robustness of inhaler bodies to become fully reusable. If inhalers are disposable there may be a rise in an increase in paper-based materials or recyclables as industry continues to understand how to deal with mixed results of take-back schemes and minimize the environmental impact of disposal. Ideally blister packs will become recyclable, reusable, or naturally degradable.
Regulation dictates the space; any new innovations still must ensure efficacy and patient safety are priority number 1. Mixed reality devices are likely to enter the consumer market, so IFUs and feedback may be transmitted in more novel ways.
Looking to the future, inhalers will lean towards a more sustainable design and standardized smaller format as patents begin to lapse, but there will be a juxtaposition between drive for lower cost devices and tech enabled devices that improve efficacy. Please get in touch to learn more or discuss how the team at HD could help responsibly accelerate your inhaler or medical device development.
Rob graduated from the Dyson School of Design Engineering at Imperial College London in 2021 with a Master’s in Design Engineering. Prior to joining HD, he worked in the automotive sector using state of the art 3D scanning and 3D printing techniques. He has a keen interest in human centred, interaction and experience design and has expertise in additive manufacturing, CAD, IoT, UI and mechatronics.

Early prototyping and user testing catch usability issues before costly mistakes, creating safer, smarter medical devices for users....

As we mark Love Your Lungs Week, we explore the latest trends shaping the inhalation industry. From advances in inhaler technology and sustainability initiatives to evolving patient needs and regulato...

Senior Design Development Engineer, Matt Holbrook shares an introduction to himself and how his first few months at Haughton Design have been....

As our newly appointed CEO enters his role, we ask him what he plans for the business in the future ahead....

Reflection from PDA Miniverse 2026: the big themes shaping medical devices, combination products and connected health....

As our Founder and Chairman retires, he reflects on building the company, the milestones along the way, and the future ahead....

Explore inside a sustainable inhaler - do reusable designs really offer an eco-friendly solution, or is there more to consider than reusability....

HD CEO Ash Ghadar shares drug delivery development insights from PDA Vienna....

Discover how Haughton Design's diverse team leverages their extensive experience to drive innovation in device development. Learn about our expertise and unique insights that ensure successful project...

Explore how commercial constraints influence innovation in businesses. Discover whether budget limits, regulations, and market pressures drive creativity or stifle progress in today's competitive land...
